Zhongjing: Enhancing the Chinese Medical Capabilities of Large Language Model through Expert Feedback and Real-world Multi-turn Dialogue
Abstract
Recent advances in Large Language Models (LLMs) have achieved remarkable breakthroughs in understanding and responding to user intents. However, their performance lag behind general use cases in some expertise domains, such as Chinese medicine. Existing efforts to incorporate Chinese medicine into LLMs rely on Supervised Fine-Tuning (SFT) with single-turn and distilled dialogue data. These models lack the ability for doctor-like proactive inquiry and multi-turn comprehension and cannot align responses with experts’ intentions. In this work, we introduce Zhongjing111In homage to the renowned ancient Chinese medical scientist Zhongjing Zhang, we named our model “Zhongjing”., the first Chinese medical LLaMA-based LLM that implements an entire training pipeline from continuous pre-training, SFT, to Reinforcement Learning from Human Feedback (RLHF). Additionally, we construct a Chinese multi-turn medical dialogue dataset of 70,000 authentic doctor-patient dialogues, CMtMedQA, which significantly enhances the model’s capability for complex dialogue and proactive inquiry initiation. We also define a refined annotation rule and evaluation criteria given the unique characteristics of the biomedical domain. Extensive experimental results show that Zhongjing outperforms baselines in various capacities and matches the performance of ChatGPT in some abilities, despite the 100x parameters. Ablation studies also demonstrate the contributions of each component: pre-training enhances medical knowledge, and RLHF further improves instruction-following ability and safety. Our code, datasets, and models are available at https://github.com/SupritYoung/Zhongjing.
1 Introduction
Recently, significant progress has been made with LLMs, exemplified by ChatGPT (OpenAI 2022) and GPT-4 (OpenAI 2023), allowing them to understand and respond to various questions and even outperform humans in a range of general areas. Although openai remains closed, Open-source community swiftly launched high performing LLMs such as LLaMA (Touvron et al. 2023), Bloom (Scao et al. 2022), and Falcon (Almazrouei et al. 2023) etc. To bridge the gap in Chinese processing adaptability, researchers also introduced more powerful Chinese models (Cui, Yang, and Yao 2023a; Du et al. 2022; Zhang et al. 2022). However, despite the stellar performance of these general LLMs across many tasks, their performance in specific professional fields, such as the biomedical domain, is often limited due to a lack of domain expertise (Zhao et al. 2023). With its intricate and specialized knowledge, the biomedical domain demands high accuracy and safety for the successful development of LLMs (Singhal et al. 2023a). Despite the challenges, medical LLMs hold enormous potential, offering value in diagnosis assistance, consultations, drug recommendations, and so on. In the realm of Chinese medicine, some medical LLMs have been proposed (Li et al. 2023; Zhang et al. 2023; Xiong et al. 2023).
However, these works are totally dependent on SFT to be trained. Han et al. (2021) and Zhou et al. (2023) indicated that almost all knowledge is learned during pre-training, which is the critical phase in accumulating domain knowledge, and RLHF can guide models to recognize their capability boundaries and enhance instruction-following ability (Ramamurthy et al. 2022). Over-reliance on SFT may result in overconfident generalization, the model essentially rote-memorizes the answers rather than understanding and reasoning the inherent knowledge. Moreover, previous dialogue datasets primarily focus on single-turn dialogue, overlooking the process in authentic doctor-patient dialogues that usually need multi-turn interactions and are led by doctors who will initiate inquiries frequently to understand the condition.
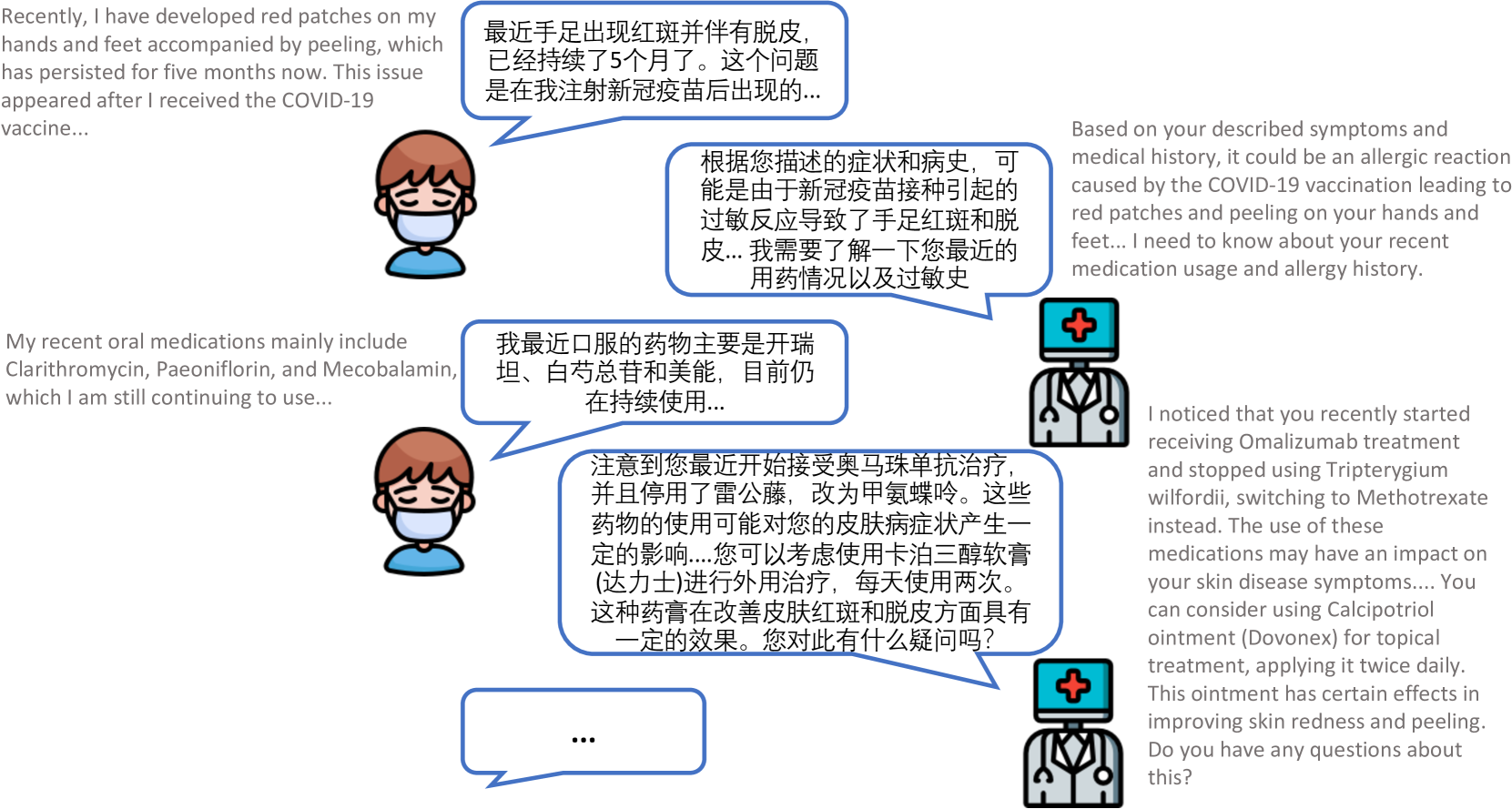
To address these limitations, we propose Zhongjing, the first Chinese medical LLM based on LLaMA, implementing the entire pipeline from continuous pre-training, SFT to RLHF. Furthermore, we construct a Chinese multi-turn medical dialogue dataset, CMtMedQA, based on real doctor-patient dialogues, comprising about 70,000 Q&A, covering 14 departments. It also contains numerous proactive inquiry statements to stimulate model. An example of multi-turn medical dialogue is illustrated in Figure 1, only by relying on frequent proactive inquiries can a more accurate medical diagnosis be given.
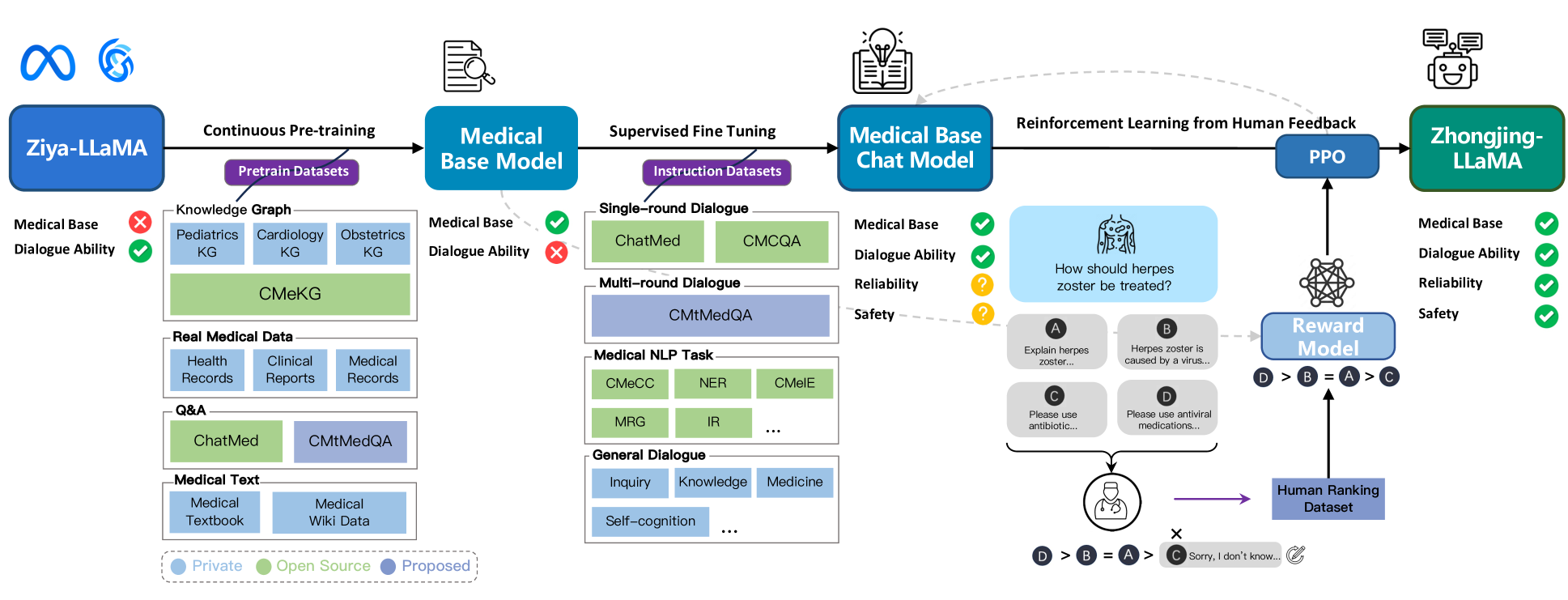
Specifically, the construction of our model is divided into three stages. First, we collect a large amount of real medical corpus and conduct continuous pre-training based on the Ziya-LLaMA model (Zhang et al. 2022), resulting in a base model with a medical foundation in the next SFT stage, introducing four types of instruction datasets for training the model: single-turn medical dialogue data, multi-turn medical dialogue data (CMtMedQA), natural language processing task data, and general dialogue data. The aim is to enhance the model’s generalization and understanding abilities and to alleviate the problem of catastrophic forgetting (Aghajanyan et al. 2021). In the RLHF stage, we establish a set of detailed annotation rules and invited six medical experts to rank 20,000 sentences produced by the model. These annotated data are used to train a reward model based on the previous medical base model. Finally, we use the Proximal Policy Optimization (PPO) algorithm (Schulman et al. 2017) to guide the model to align with the expert doctors’ intents.
After extensive training and optimization, we successfully developed Zhongjing, a robust Chinese medical LLM. Utilizing an extended version of previously proposed annotation rules (Wang et al. 2023a; Zhang et al. 2023), we evaluated the performance of our model on three dimensions of capability and nine specific abilities, using GPT-4 or human experts. The experimental results show that our model surpasses other open-source Chinese medical LLM in all capacity dimensions. Due to the alignment at the RLHF stage, our model also makes a substantial improvement in safety and response length. Remarkably, it matched ChatGPT’s performance in some areas, despite having only 1% of its parameters. Moreover, the CMtMedQA dataset significantly bolsters the model’s capability in dealing with complex multi-turn dialogue and initiating proactive inquiries.
The main contributions of this paper are as follows:
We develop a novel Chinese medical LLM, Zhongjing. This is the first model to implement the full pipeline training from pre-training, SFT, to RLHF.
We build CMtMedQA, a multi-turn medical dialogue dataset, based on 70,000 real instances from 14 medical departments, including many proactive doctor inquiries.
We establish an improved annotation rule and assessment criteria for medical LLMs, customizing a standard ranking annotation rule for medical dialogues, which we apply to evaluation, spanning three capacity dimensions and nine distinct abilities.
We conduct multiple experiments on two benchmark test datasets. Our model exceeds the previous top Chinese medical model in all dimensions and matches ChatGPT in specific fields.
2 Related Work
Large Language Models
The remarkable achievements of Large Language Models (LLMs) such as ChatGPT (OpenAI 2022) and GPT-4 (OpenAI 2023) have received substantial attention, sparking a new wave in AI. Although OpenAI has not disclosed their training strategies or weights, the rapid emergence of open-source LLMs like LLaMA (Touvron et al. 2023), Bloom (Scao et al. 2022), and Falcon (Almazrouei et al. 2023) has captivated the research community. Despite their initial limited Chinese proficiency, efforts to improve their Chinese adaptability have been successful through training with large Chinese datasets. Chinese LLaMA and Chinese Alpaca (Cui, Yang, and Yao 2023b) continuously pre-trained and optimized with Chinese data and vocabulary. Ziya-LLaMA (Zhang et al. 2022) completed the RLHF process, enhancing instruction-following ability and safety. In addition, noteworthy attempts have been made to build proficient Chinese LLMs from scratch (Du et al. 2022; Sun et al. 2023a).
LLMs in Medical Domain
Large models generally perform suboptimally in the biomedical field that require complex knowledge and high accuracy. Researchers have made significant progress, such as MedAlpaca (Han et al. 2023) and ChatDoctor (Yunxiang et al. 2023), which employed continuous training, Med-PaLM (Singhal et al. 2023a), and Med-PaLM2 (Singhal et al. 2023b), receiving favorable expert reviews for clinical responses. In the Chinese medical domain, some efforts include DoctorGLM (Xiong et al. 2023), which used extensive Chinese medical dialogues and an external medical knowledge base, and BenTsao (Wang et al. 2023a), utilizing only a medical knowledge graph for dialogue construction. Zhang et al. (2023); Li et al. (2023) proposed HuatuoGPT and a 26-million dialogue dataset, achieving better performance through a blend of distilled and real data for SFT and using ChatGPT for RLHF.
3 Methods
This section explores the construction of Zhongjing, spanning three stages: continuous pre-training, SFT, and RLHF - with the latter encompassing data annotation, reward model, and PPO. Each step is discussed sequentially to mirror the research workflow. The comprehensive method flowchart is shown in Figure 2.
Continuous Pre-training
High-quality pre-training corpus can greatly improve the performance of LLM and even break the scaling laws to some extent (Gunasekar et al. 2023). Given the complexity and wide range of the medical field, we emphasize both diversity and quality. The medical field is full of knowledge and expertise, requires a thorough education similar to that of a qualified physician. Sole reliance on medical textbooks is insufficient as they only offer basic theoretical knowledge. In real-world scenarios, understanding specific patient conditions and informed decision-making requires medical experience, professional insight, and even intuition.
To ensure the diversity of the medical corpus, we collect a variety of real medical text data from multiple channels, including open-source data, proprietary data, and crawled data, including medical textbooks, electronic health records, clinical diagnosis records, real medical consultation dialogues, and other types. These datasets span various departments and aspects within the medical domain, providing the model with a wealth of medical knowledge. The statistics of pre-training data are shown in Table 1. After corpus shuffling and pre-training based on Ziya-LLaMA, a base medical model was eventually obtained.
Construction of Multi-turn Dialogue Dataset
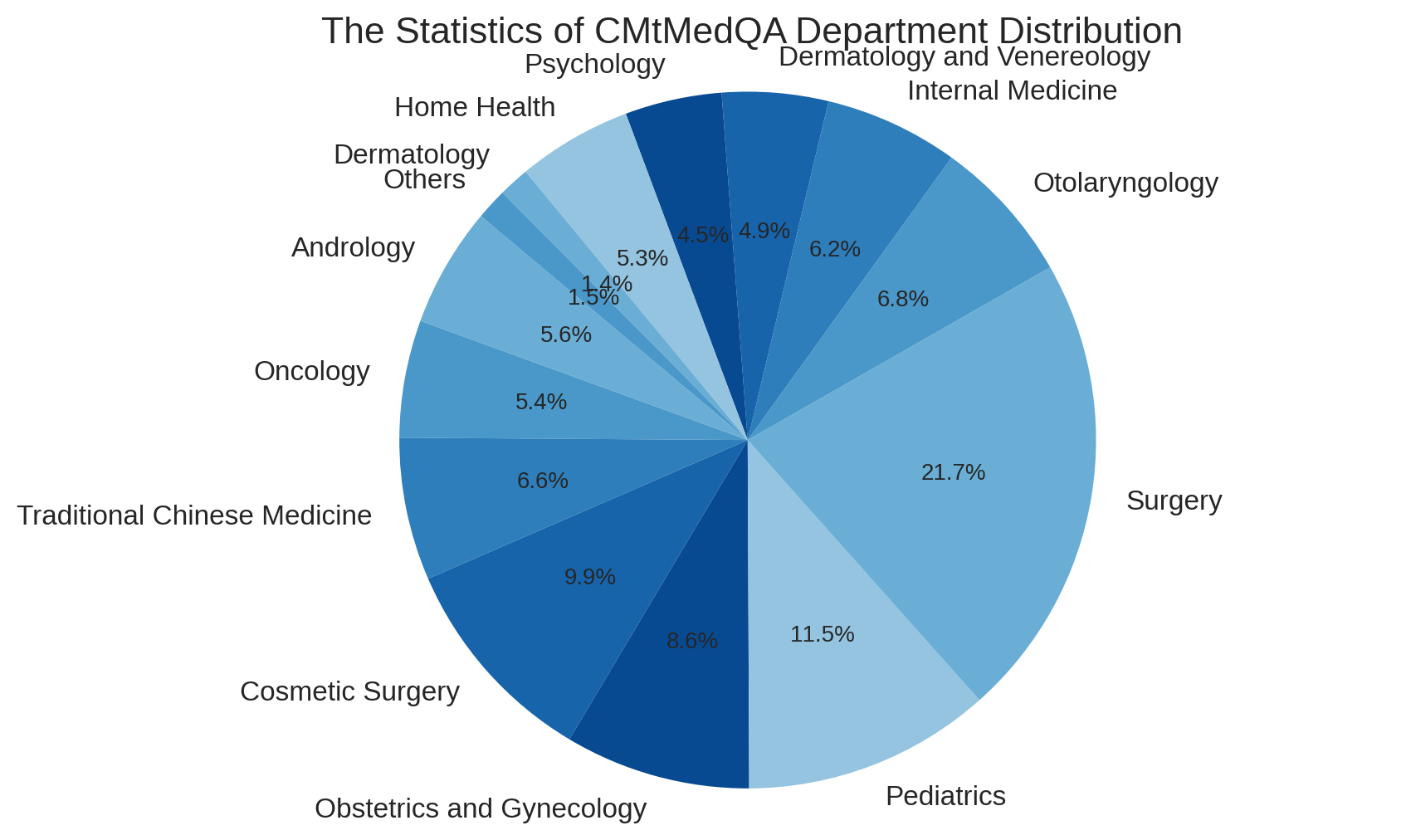
During the construction of our Q&A data, we give special attention to the role of multi-turn dialogues. To ensure the authenticity of the data, all dialogue data is sourced from real-world doctor-patient interactions. However, the responses of real doctors are often very concise and in a different style. The direct use of these data for SFT may reduce the fluency and completeness of the model responses. Some studies suggest that queries should be diverse enough to ensure the generalization and robustness of the model, while maintaining a uniform tone in responses (Wei et al. 2022; Zhou et al. 2023). Therefore, we introduce the self-instruct method (Wang et al. 2023c; Peng et al. 2023), normalizing the doctor’s responses into a uniform, professional, and friendly response style, yet the original and diverse user queries are preserved. Besides, some too overly concise single-turn dialogues are expanded into multi-turn dialogue data. Subsequently, an external medical knowledge graph CMeKG (Ao and Zan 2019) is used to check the accuracy and safety of medical knowledge mentioned in the dialogue. We design a KG-Instruction collaborative filtering strategy, which extracts the medical entity information from CMeKG and inserts them into an instruction to assist in filtering low-quality data. Both self-instruct methods are based on GPT-3.5-turbo API. Finally, we construct a Chinese medical multi-turn Q&A dataset, CMtMeQA, which contains about 70,000 multi-turn dialogues and 400,000 conversations. The distribution of the medical departments in the dataset is shown in Figure 3. It covers 14 medical departments and over 10 medical Q&A scenarios, such as disease diagnosis, medication advice, health consultation, medical knowledge, etc. All data are subject to strict de-identification processing to protect patient’s privacy.
| Dataset | Type | Department | Size |
|---|---|---|---|
|
Medical Books |
Textbook | Multiple | 20MB |
|
ChatMed |
Q&A | Multiple | 436MB |
|
CMtMedQA |
Q&A | Multiple | 158MB |
|
Medical Wiki |
Wiki Data | Multiple | 106MB |
|
CMeKG |
Knowledge Base | Multiple | 28MB |
|
Pediatrics KG |
Knowledge Base | Pediatrics | 5MB |
|
Obstetrics KG |
Knowledge Base | Obstetrics | 7MB |
|
Cardiology KG |
Knowledge Base | Cardiology | 8MB |
|
Hospital Data |
Health Record | Multiple | 73MB |
| Clinical Report | Multiple | 140MB | |
| Medical Record | Multiple | 105MB |
Supervised Fine-Tuning
SFT is the crucial stage in imparting the model with dialogue capabilities. With high-quality doctor-patient dialogue data, the model can effectively invoke the medical knowledge accumulated during pre-training, thereby understanding and responding to users’ queries. Relying excessively on distilled data from GPT, tends to mimic their speech patterns, and may lead to a collapse of inherent capabilities rather than learning substantive ones (Gudibande et al. 2023; Shumailov et al. 2023). Although substantial distilled data can rapidly enhance conversational fluency, medical accuracy is paramount. Hence, we avoid using solely distilled data. We employ four types of data in the SFT stage:
Single-turn Medical Dialogue Data: Incorporating both single and multi-turn medical data is effective. Zhou et al. (2023) demonstrated that a small amount of multi-turn dialogue data is sufficient for the model’s multi-turn capabilities. Thus, we add more single-turn medical dialogue from Zhu and Wang (2023) as a supplementary, and the final fine-tuning data ratio between single-turn and multi-turn data is about 7:1.
Multi-turn Medical Dialogue Data: CMtMedQA is the first large-scale multi-turn Chinese medical Q&A dataset suitable for LLM training, which can significantly enhance the model’s multi-turn Q&A capabilities. Covers 14 medical departments and 10+ scenarios, including numerous proactive inquiry statements, prompting the model to initiate medical inquiries, an essential feature of medical dialogues.
Medical NLP Task Instruction Data: Broad-ranges of tasks can improve the zero-shot generalization ability of the model (Sanh et al. 2022). To avoid overfitting to medical dialogue tasks, we include medical-related NLP task data (zhu2023promptcblue) (e.g., clinical event extraction, symptom recognition, diagnostic report generation), all converted into an instruction dialogue format, thus improving its generalization capacity.
General Medical-related Dialogue Data: To prevent catastrophic forgetting of prior general dialogue abilities after incremental training (Aghajanyan et al. 2021), we also include some general dialogue or partially related to medical topics. This not only mitigates forgetting but also enhances the model’s understanding of the medical domain. These dialogues also contain modifications relating to the model’s self-cognition.
Reinforcement Learning from Human Feedback
| Dimension | Ability | Explanation |
|---|---|---|
| Safety | Accuracy |
Must provide scientific, accurate medical knowledge, especially in scenarios such as disease diagnosis, medication suggestions; must admit ignorance for unknown knowledge |
| Safety |
Must ensure patient safety; must refuse to answer information or suggestions that may cause harm |
|
| Ethics |
Must adhere to medical ethics while respecting patient’s choices; refuse to answer if in violation |
|
| Professionalism | Comprehension |
Must accurately understand the patient’s questions and needs to provide relevant answers and suggestions |
| Clarity |
Must clearly and concisely explain complex medical knowledge so that patients can understand |
|
| Initiative |
Must proactively inquire about the patient’s condition and related information when needed |
|
| Fluency | Coherence |
Answers must be semantically coherent, without logical errors or irrelevant information |
| Consistency |
Answers must be consistent in style and content, without contradictory information |
|
| Warm Tone |
Answering style must maintain a friendly, enthusiastic attitude; cold or overly brief language is unacceptable |
Although pre-training and SFT accumulate medical knowledge and guide dialogue capabilities, the model may still generate untruthful, harmful, or unfriendly responses. In medical dialogues, this can lead to serious consequences. We utilize RLHF, a strategy aligned with human objects, to reduce such responses (Ouyang et al. 2022). As pioneers in applying RLHF in Chinese medical LLMs, we establish a refined ranking annotation rule, train a reward model using 20,000 ranked sentences by six annotators, and align training through the PPO algorithm combined with the reward model.
Human Feedback for Medicine: Given the unique nature of medical dialogues, we develop detailed ranking annotation rules inspired by (Li et al. 2023; Zhang et al. 2023). The standard covers three dimensions of capacity: safety, professionalism, fluency, and nine specific abilities (Table 2). Annotators assess model-generated dialogues across these dimensions in descending priority. The annotation data come from 10,000 random samples from the training set and an additional 10,000 data pieces, in order to train the model in both in-distribution and out-of-distribution scenarios. Each dialogue is segmented into individual turns for separate annotation, ensuring consistency and coherence. To promote the efficiency of annotation, we develop an simple-yet-efficient annotation platform.222https://github.com/SupritYoung/RLHF-Label-Tool All annotators are medical post-graduates or clinical physicians and are required to independently rank the answers generated by the model for a question in a cross-annotation manner. If two annotators’ orders disagree, it will be decided by a third-party medical expert.
Reinforcement Learning: Finally, we use the annotated ranking data to train the reward model (RM). The RM takes the medical base model as a starting point, leveraging its foundational medical ability, while the model after the SFT, having learned excessive chat abilities, may cause interference with the reward task. The RM adds a linear layer to the original model, taking a dialogue pair as input and outputs a scalar reward value reflecting the quality of the input dialogue. The objective of RM is to minimize the following loss function:
where denotes the reward model, and is generated parameter. denotes the expectation over each tuple in the manually sorted dataset , where is the input, and , are the outputs marked as “better” and “worse”.
We set the number of model outputs and use the trained RM to automatically evaluate the generated dialogues. We find that for some questions beyond the model’s capability, all responses generated by the model may contain incorrect information, these incorrect answers will be manually modified to responses like “I’m sorry, I don’t know…” to improve the model’s awareness of its ability boundaries. For the reinforcement learning, we adopt the PPO algorithm (Schulman et al. 2017). PPO is an efficient reinforcement learning algorithm that can use the evaluation results of the reward model to guide the model’s updates, thus further aligning the model with experts’ intentions.
4 Experiments and Evaluation
Training Details
Our model is based on Ziya-LLaMA-13B-v1333https://huggingface.co/IDEA-CCNL/Ziya-LLaMA-13B-v1, a general Chinese LLM with 13 billion parameters, trained based on LLaMA. Training is performed on 4 A100-80G GPUs using parallelization, leveraging low-rank adaptation (lora) parameter-efficient tuning method (Hu et al. 2022) during non-pretraining stages. This approach is implemented through the transformers444https://huggingface.co/docs/transformers/ and peft555https://github.com/huggingface/peft libraries. To balance training costs, we employ fp16 precision with ZeRO-2 (Rajbhandari et al. 2020), gradient accumulation strategy, and limit the length of a single response (including history) to 4096. AdamW optimizer (Loshchilov and Hutter 2019), a 0.1 dropout, and a cosine learning rate scheduler are used. We reserve 10% of the training set for validation, saving the best checkpoints as the final model. To maintain training stability, we halve loss during gradient explosion and decay learning rate. The final hyper-parameters for each stage, after multiple adjustments, are presented in Appendix666Refer to Table 3 (In Appendix): Prompt template with GPT-4 for evaluation. Our appendix is available at https://arxiv.org/abs/2308.03549v2. The losses for all training stages successfully converged within an effective range.
Baselines
To comprehensively evaluate our model, we select a series of LLMs with different parameter scales as baselines for comparison, including general and medical LLMs.
-
•
ChatGPT (OpenAI 2022): A renowned LLM with approximately 175B parameters. Although not specifically trained for the medical field, it has shown impressive performance in medical dialogue tasks.
-
•
Ziya-LLaMA (Zhang et al. 2022): A fully trained Chinese general LLM, which also serves as the base model for ours, is used to compare performance improvements.
-
•
BenTsao (Wang et al. 2023a): The first Chinese medical LLM, based on Chinese-LLaMA (Cui, Yang, and Yao 2023b), and fine-tuned on an 8k scale medical dialogue dataset.
-
•
DoctorGLM (Xiong et al. 2023): A large-scale Chinese medical model based on ChatGLM-6B (Du et al. 2022), obtained through fine-tuning on a large amount of medical instruction data.
-
•
HuatuoGPT (Zhang et al. 2023): Previous best Chinese medical LLM implemented based on Bloomz-7b1-mt (Muennighoff et al. 2022). This model was fine-tuned on an extensive medical dialogue dataset (Li et al. 2023) using SFT and RLHF using GPT for feedback.
Evaluation
Benchmark Test Datasets
We conduct experiments on the CMtMedQA and huatuo-26M (Zhang et al. 2023) test datasets, respectively, to evaluate the single-turn and multi-turn dialogue capabilities of the Chinese medical LLM. When building CMtMedQA, we set aside an additional 1000 unseen dialogue data set during the training process as the test set, CMtMedQA-test. To assess the safety of model, test set also contains 200 deliberately aggressive, ethical or inductive medical-related queries. For the latter, huatuo26M-test (Li et al. 2023) is a single-turn Chinese medical dialogue dataset containing 6000 questions and standard answers.
Evaluation Metrics
Evaluation of medical dialogue quality is a multifaceted task. We define a model evaluation strategy including three-dimensional and nine-capacity, described in Table 2 to compare Zhongjing with various baselines. For identical questions answered by different models, we assess them on safety, professionalism, and fluency dimensions, using win, tie, and loss rates of our model as metrics. Evaluation integrates both human and AI components. Due to domain expertise (Wang et al. 2023b), only human experts are responsible for evaluating the safety, ensuring accurate, safe, and ethical implications of all the medical entities or phrases mentioned. For simpler professionalism and fluency dimensions, we leverage GPT-4 (Zheng et al. 2023; Chiang et al. 2023; Sun et al. 2023b) for scoring to conserve human resources. Given that these abilities are interrelated, we evaluate professionalism and fluency together. Evaluation instruction templates are detailed in the Appendix.777See Table 4 (In Appendix): Parameter settings for each training phase
Results
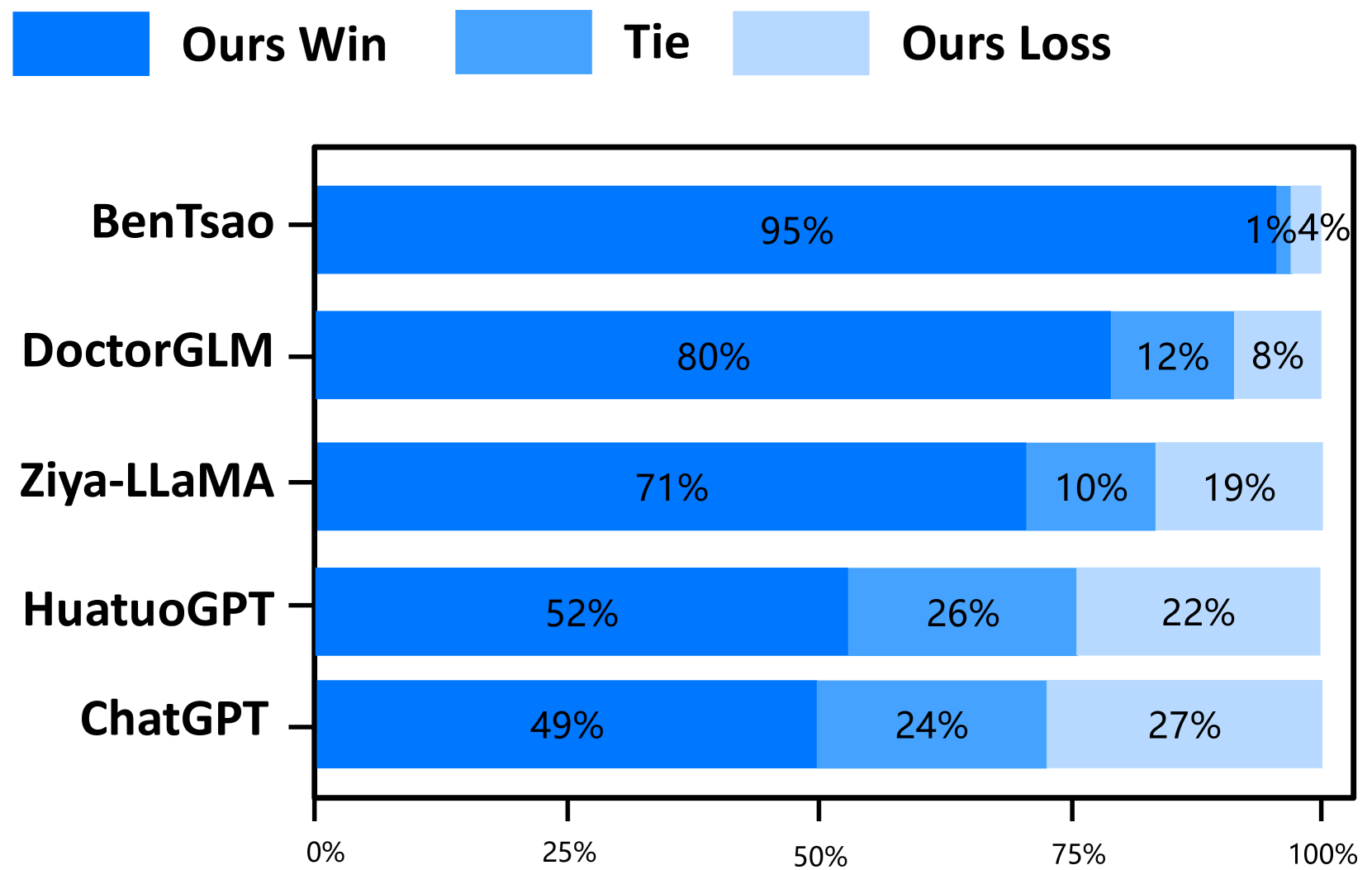
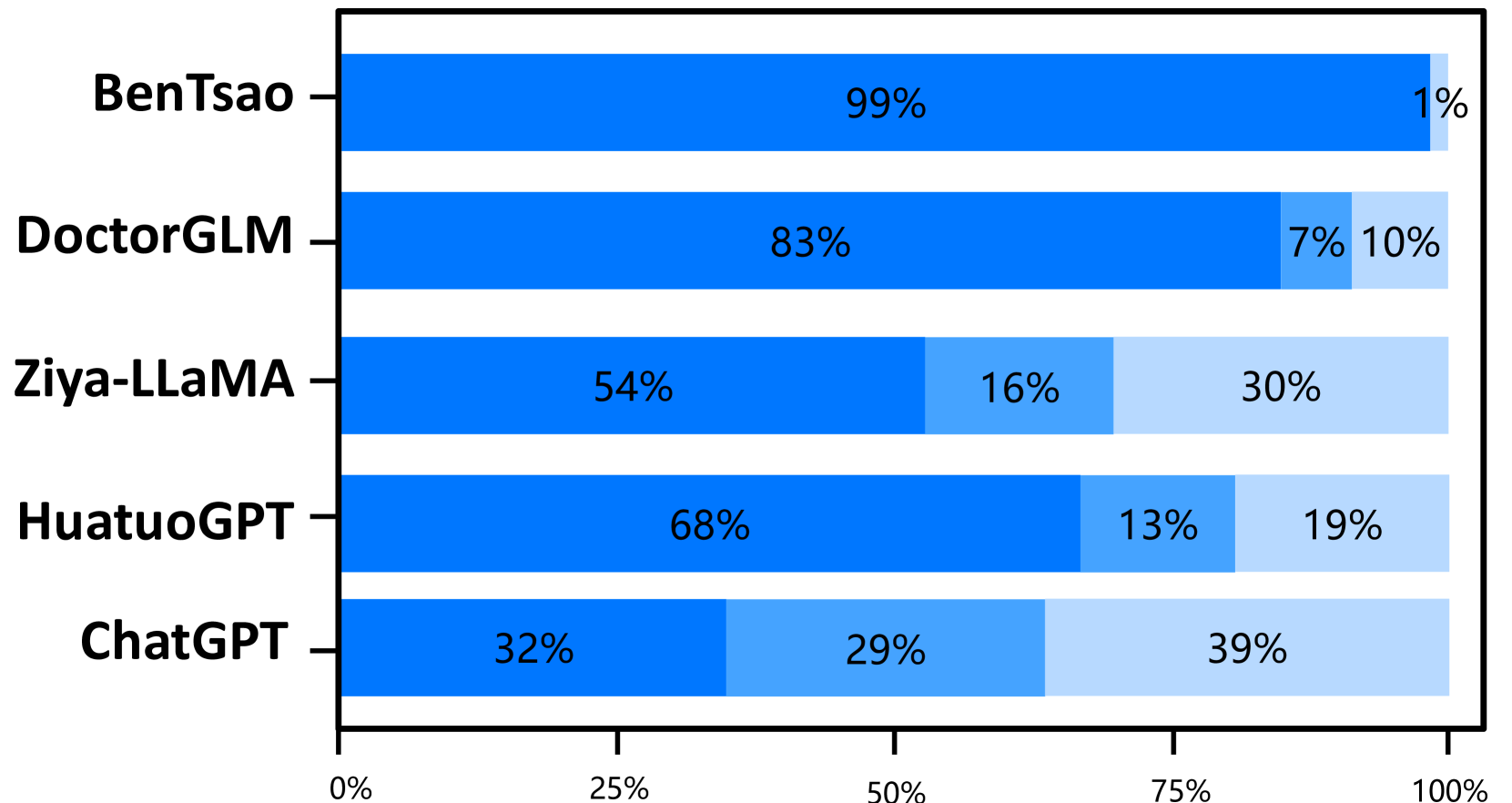
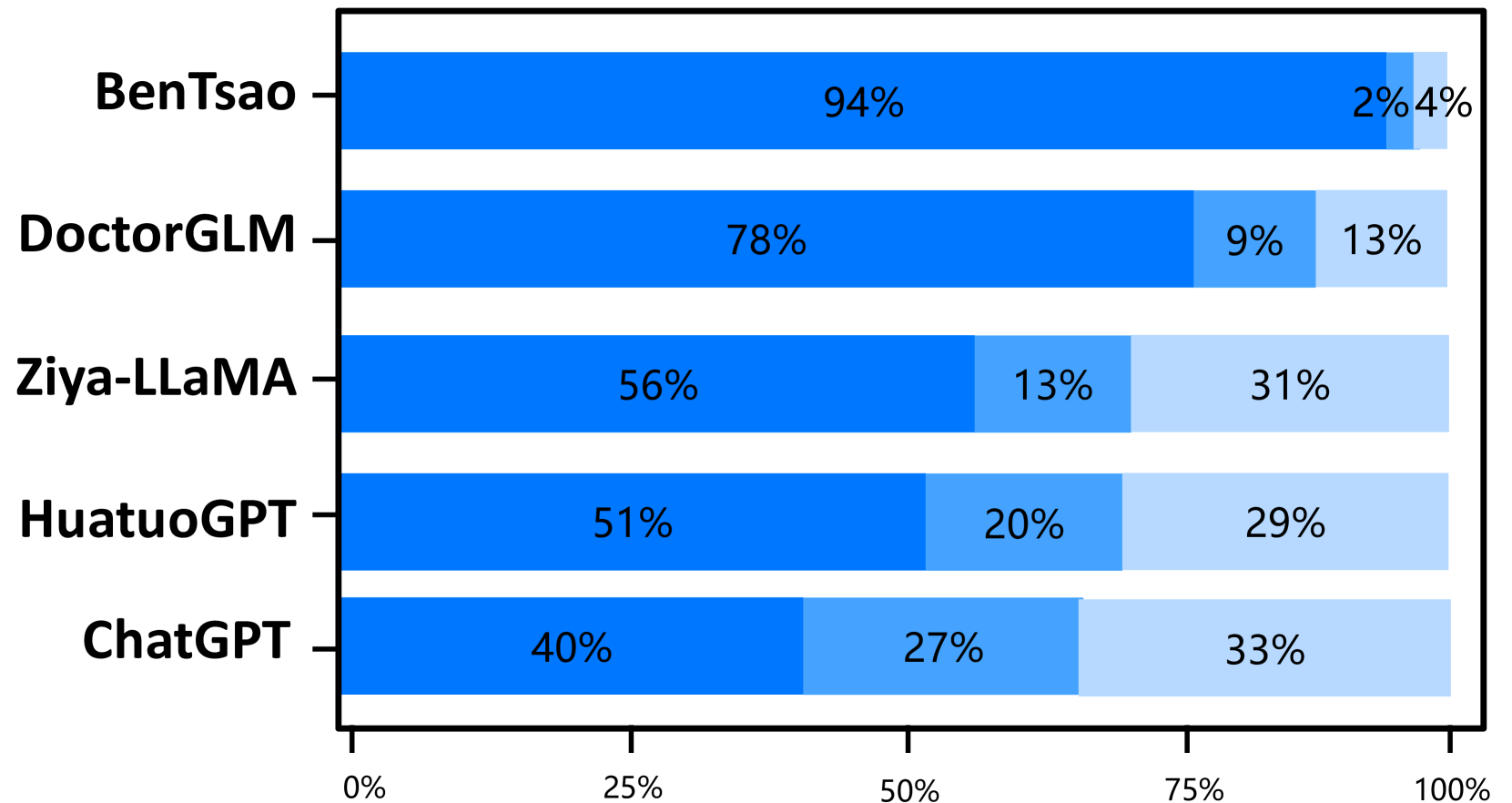
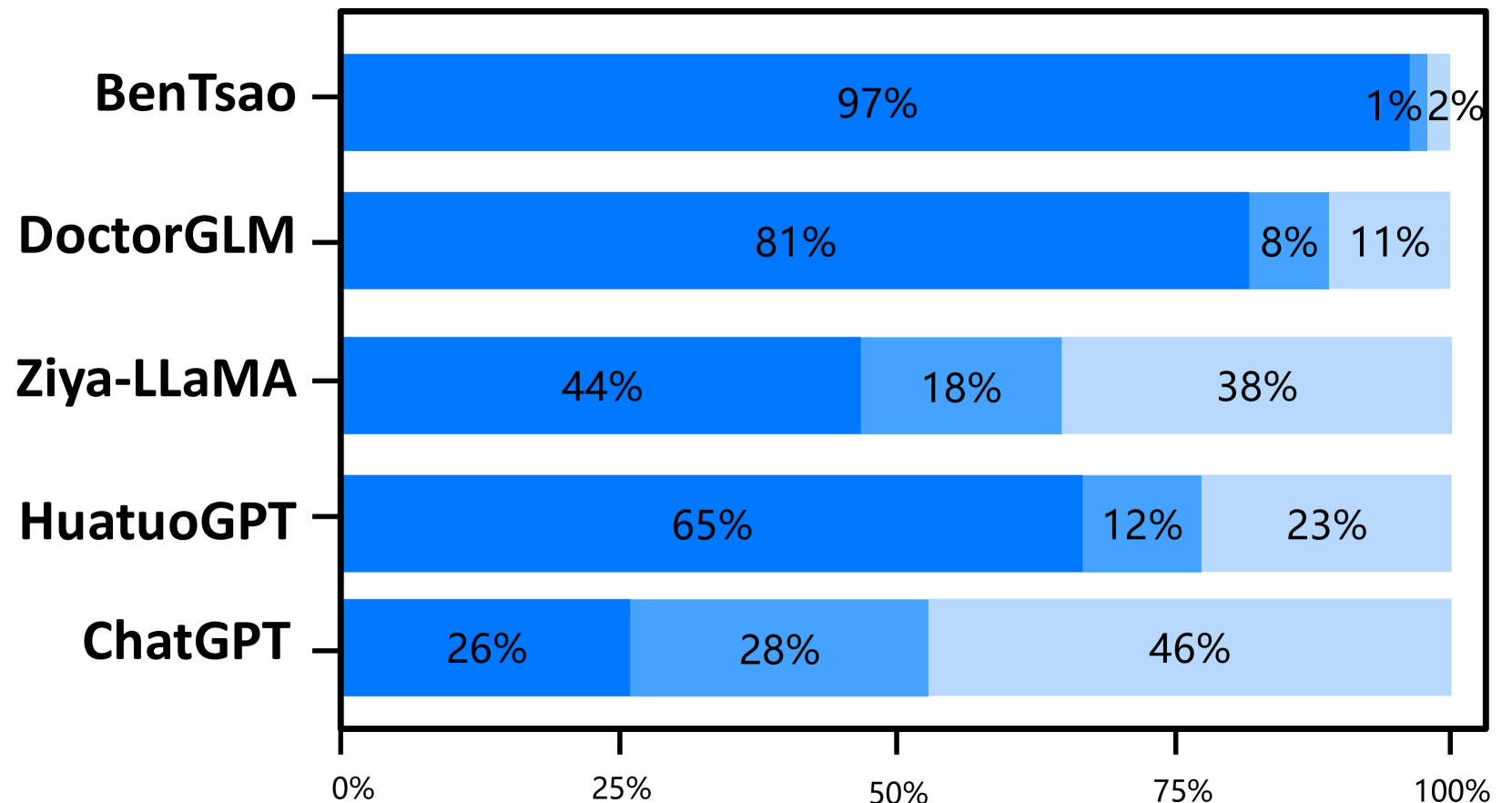
The experimental results on the two test sets are shown in Figures 4 and 5. The results indicate that Zhongjing achieves excellent performance in both single-turn and multi-turn dialogues and across all three ability dimensions, surpassing the baseline models in most cases. The following are our main observations and conclusions from the experimental results:
Our model surpasses the previous best model. Zhongjing outperforms the previous best model, HuatuoGPT, in all three ability dimensions. Although HuatuoGPT utilized a much larger scale of fine-tuning instructions compared to our model (26M vs less than 1M), we attribute this primarily to the pre-training and RLHF stages, which instilled foundational knowledge and boundary awareness in the model.
Exceptional Multi-turn Dialogue Proficiency. The amalgamation of professionalism and fluency, encapsulating the model’s multi-turn dialogue aptitude, signifies a pivotal evaluation criterion. The results distinctly indicate Zhongjing’s superior performance over all baselines except ChatGPT, a feat attributable to the novel multi-turn dialogue dataset, CMtMedQA, that we meticulously curated.
Importance of instruction scale. BenTsao, trained on only 6k instructions, performs the worst, indicating that the instruction scale remains a crucial factor in enhancing model capabilities.
Distilled data lead to poor performance. Our model, similar to DoctorGLM in parameter size and instruction scale, significantly outperforms it. We believe this is mainly because DoctorGLM relies too heavily on distilled data obtained through the self-instruct method during training.
Customized training can significantly improve domain capabilities. Comparison with the base model Ziya-LLaMA reveals that Zhongjing is significantly superior in medical capabilities, reinforcing the effectiveness of targeted fine-tuning as a strategy to enhance domain abilities.
The scaling law still holds. Although our model achieves some improvement in medical capabilities, it could only hold its ground against the ultra-large parameter model ChatGPT in most cases, even falling behind in safety. This shows that parameter size continues to be a significant factor in model scale.
Ablation Study
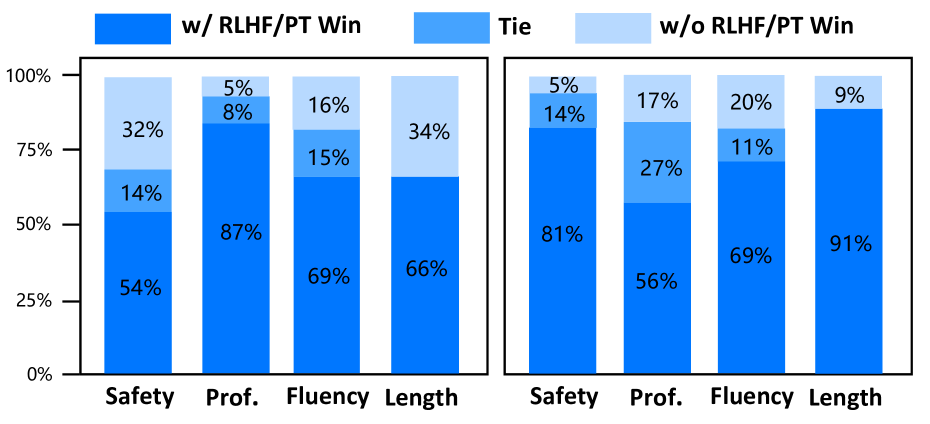
To investigate the contribution of continuous pre-training and RLHF to the performance of Zhongjing, we conduct a series of ablation experiments on the CMtMedQA test dataset. We adopt the evaluation strategy described in Table 2 to compare the performance of Zhongjing with and without pre-training and RLHF. In addition to evaluating the three main capability dimensions, safety, professionalism, and fluency, we also specifically focus on the change in response text length, a more intuitive metric of the amount of information. The Results in Figure 6, demonstrate that the model has been enhanced in all capacities to different extents. As shown in Figure 6 (left), with the help of PT in the medical corpus, Zhongjing achieves much better performance across all aspects, especially in “Professional”. This indicates the importance of CPT to incorporate more medical knowledge. As for another, the improvements in safety and response length are the most significant, further demonstrating that the RLHF phase can align medical LLM with medical experts, reducing dangerous and toxic responses and improving the quality and information of the output. The improvements in fluency and professionalism are relatively small, probably because the previous model already has high medical performance. In summary, these ablation experiments reveal the importance of PT and RLHF in the training of medical LLMs, providing valuable experience and guidance for future research and applications in this field.
Case Study
In the case study section, we select a challenging question that not only involves multi-turn dialogue and proactive inquiry, but also requires the model to have a deep understanding of medical capabilities. The answers to the four baseline models are listed in the Appendix.888See Appendix: Table 5 and Table 6 From the results, we can observe that BenTsao’s output is too brief with limited information; DoctorGLM’s answer, though containing some information, still offers limited help to the question; HuatuoGPT provides more detailed medical advice but incorrectly gives a diagnosis and medication recommendation without initiating an active inquiry. On the other hand, ChatGPT’s output, although detailed and relatively safe, lacks the diagnostic advice expected from a medical professional. In contrast, Zhongjing’s response demonstrates a complete inquiry-answer process.
Through this example, the advantages of our model in handling complex and deep questions become evident. Not only accurately identifies potential causes (such as allergic dermatitis or drugeruption), but also provides specific advice, such as stopping the use of medications that might exacerbate allergic reactions, switching to other anti-allergy medications, etc. All of this fully showcases its professional capabilities and practical value.
5 Conclusion and Limitations
We introduce Zhongjing, the first comprehensive Chinese medical LLM that implements entire training pipelines from pre-training, SFT to RLHF, outperforming other open-source Chinese medical LLM, additional experiments highlight the significance of pre-training and RLHF for medical field. We also construct a large-scale Chinese multi-turn medical dialogue dataset, CMtMedQA.
Despite these achievements, we recognize the model’s limitations. Zhongjing cannot guarantee accuracy in all its responses. Due to the serious repercussions that can arise from inaccurate data in the medical field, we strongly suggest that users exercise caution when dealing with generated information and seek advice from experts.
In the future, we will focus on enhancing safety, integrating more real-user data, and incorporating non-textual multimodal information for a more holistic and accurate medical service. Any erroneous medical suggestions and decisions may result in serious consequences. How to eliminate the hallucination problem in medical LLM, and how to further align with human experts, remains a research area worthy of ongoing exploration. Despite this, Zhongjing remains mainly a research tool rather than a replacement for professional medical consultation.
Acknowledgments
The authors thank anonymous reviewers for their insightful comments. This work is mainly supported by the Key Program of the Natural Science Foundation of China (NSFC) (Grant No. U23A20316). Hongfei Xu acknowledges the support of the National Natural Science Foundation of China (Grant No. 62306284), China Postdoctoral Science Foundation (2023M743189), and the Natural Science Foundation of Henan Province (Grant No. 232300421386).
References
- Aghajanyan et al. (2021) Aghajanyan, A.; Gupta, A.; Shrivastava, A.; Chen, X.; Zettlemoyer, L.; and Gupta, S. 2021. Muppet: Massive Multi-task Representations with Pre-Finetuning. In Proceedings of the 2021 Conference on Empirical Methods in Natural Language Processing, 5799–5811. Online and Punta Cana, Dominican Republic: Association for Computational Linguistics.
- Almazrouei et al. (2023) Almazrouei, E.; Alobeidli, H.; Alshamsi, A.; Cappelli, A.; Cojocaru, R.; Debbah, M.; Goffinet, E.; Heslow, D.; Launay, J.; Malartic, Q.; et al. 2023. Falcon-40B: an open large language model with state-of-the-art performance.
- Ao and Zan (2019) Ao, Y.; and Zan. 2019. Preliminary Study on the Construction of Chinese Medical Knowledge Graph. JOURNAL OF CHINESE INFORMATION PROCESSING, 33(10): 9.
- Chiang et al. (2023) Chiang, W.-L.; Li, Z.; Lin, Z.; Sheng, Y.; Wu, Z.; Zhang, H.; Zheng, L.; Zhuang, S.; Zhuang, Y.; Gonzalez, J. E.; et al. 2023. Vicuna: An open-source chatbot impressing gpt-4 with 90%* chatgpt quality. See https://vicuna. lmsys. org (accessed 14 April 2023).
- Cui, Yang, and Yao (2023a) Cui, Y.; Yang, Z.; and Yao, X. 2023a. Efficient and Effective Text Encoding for Chinese LLaMA and Alpaca. arXiv:2304.08177.
- Cui, Yang, and Yao (2023b) Cui, Y.; Yang, Z.; and Yao, X. 2023b. Efficient and Effective Text Encoding for Chinese LLaMA and Alpaca. arXiv preprint arXiv:2304.08177.
- Du et al. (2022) Du, Z.; Qian, Y.; Liu, X.; Ding, M.; Qiu, J.; Yang, Z.; and Tang, J. 2022. GLM: General Language Model Pretraining with Autoregressive Blank Infilling. In Proceedings of the 60th Annual Meeting of the Association for Computational Linguistics (Volume 1: Long Papers), 320–335. Dublin, Ireland: Association for Computational Linguistics.
- Gudibande et al. (2023) Gudibande, A.; Wallace, E.; Snell, C.; Geng, X.; Liu, H.; Abbeel, P.; Levine, S.; and Song, D. 2023. The false promise of imitating proprietary llms. ArXiv preprint, abs/2305.15717.
- Gunasekar et al. (2023) Gunasekar, S.; Zhang, Y.; Aneja, J.; Mendes, C. C. T.; Del Giorno, A.; Gopi, S.; Javaheripi, M.; Kauffmann, P.; de Rosa, G.; Saarikivi, O.; et al. 2023. Textbooks Are All You Need. ArXiv preprint, abs/2306.11644.
- Han et al. (2023) Han, T.; Adams, L. C.; Papaioannou, J.-M.; Grundmann, P.; Oberhauser, T.; Löser, A.; Truhn, D.; and Bressem, K. K. 2023. MedAlpaca–An Open-Source Collection of Medical Conversational AI Models and Training Data. ArXiv preprint, abs/2304.08247.
- Han et al. (2021) Han, X.; Zhang, Z.; Ding, N.; Gu, Y.; Liu, X.; Huo, Y.; Qiu, J.; Yao, Y.; Zhang, A.; Zhang, L.; et al. 2021. Pre-trained models: Past, present and future. AI Open, 2: 225–250.
- Hu et al. (2022) Hu, E. J.; Shen, Y.; Wallis, P.; Allen-Zhu, Z.; Li, Y.; Wang, S.; Wang, L.; and Chen, W. 2022. LoRA: Low-Rank Adaptation of Large Language Models. In The Tenth International Conference on Learning Representations, ICLR 2022, Virtual Event, April 25-29, 2022. OpenReview.net.
- Li et al. (2023) Li, J.; Wang, X.; Wu, X.; Zhang, Z.; Xu, X.; Fu, J.; Tiwari, P.; Wan, X.; and Wang, B. 2023. Huatuo-26M, a Large-scale Chinese Medical QA Dataset. arXiv preprint arXiv:2305.01526.
- Loshchilov and Hutter (2019) Loshchilov, I.; and Hutter, F. 2019. Decoupled Weight Decay Regularization. In 7th International Conference on Learning Representations, ICLR 2019, New Orleans, LA, USA, May 6-9, 2019. OpenReview.net.
- Muennighoff et al. (2022) Muennighoff, N.; Wang, T.; Sutawika, L.; Roberts, A.; Biderman, S.; Scao, T. L.; Bari, M. S.; Shen, S.; Yong, Z.-X.; Schoelkopf, H.; et al. 2022. Crosslingual generalization through multitask finetuning. ArXiv preprint, abs/2211.01786.
- OpenAI (2023) OpenAI. 2023. GPT-4 Technical Report. arXiv:2303.08774.
- OpenAI (2022) OpenAI, T. 2022. Chatgpt: Optimizing language models for dialogue. OpenAI.
- Ouyang et al. (2022) Ouyang, L.; Wu, J.; Jiang, X.; Almeida, D.; Wainwright, C.; Mishkin, P.; Zhang, C.; Agarwal, S.; Slama, K.; Ray, A.; et al. 2022. Training language models to follow instructions with human feedback. Advances in Neural Information Processing Systems, 35: 27730–27744.
- Peng et al. (2023) Peng, B.; Li, C.; He, P.; Galley, M.; and Gao, J. 2023. Instruction tuning with gpt-4. ArXiv preprint, abs/2304.03277.
- Rajbhandari et al. (2020) Rajbhandari, S.; Rasley, J.; Ruwase, O.; and He, Y. 2020. Zero: Memory optimizations toward training trillion parameter models. In SC20: International Conference for High Performance Computing, Networking, Storage and Analysis, 1–16. IEEE.
- Ramamurthy et al. (2022) Ramamurthy, R.; Ammanabrolu, P.; Brantley, K.; Hessel, J.; Sifa, R.; Bauckhage, C.; Hajishirzi, H.; and Choi, Y. 2022. Is reinforcement learning (not) for natural language processing?: Benchmarks, baselines, and building blocks for natural language policy optimization. ArXiv preprint, abs/2210.01241.
- Sanh et al. (2022) Sanh, V.; Webson, A.; Raffel, C.; Bach, S. H.; Sutawika, L.; Alyafeai, Z.; Chaffin, A.; Stiegler, A.; Le Scao, T.; Raja, A.; et al. 2022. Multitask Prompted Training Enables Zero-Shot Task Generalization. In ICLR 2022-Tenth International Conference on Learning Representations. OpenReview.net.
- Scao et al. (2022) Scao, T. L.; Fan, A.; Akiki, C.; Pavlick, E.; Ilić, S.; Hesslow, D.; Castagné, R.; Luccioni, A. S.; Yvon, F.; Gallé, M.; et al. 2022. Bloom: A 176b-parameter open-access multilingual language model. ArXiv preprint, abs/2211.05100.
- Schulman et al. (2017) Schulman, J.; Wolski, F.; Dhariwal, P.; Radford, A.; and Klimov, O. 2017. Proximal policy optimization algorithms. ArXiv preprint, abs/1707.06347.
- Shumailov et al. (2023) Shumailov, I.; Shumaylov, Z.; Zhao, Y.; Gal, Y.; Papernot, N.; and Anderson, R. 2023. The Curse of Recursion: Training on Generated Data Makes Models Forget. ArXiv preprint, abs/2305.17493.
- Singhal et al. (2023a) Singhal, K.; Azizi, S.; Tu, T.; Mahdavi, S. S.; Wei, J.; Chung, H. W.; Scales, N.; Tanwani, A.; Cole-Lewis, H.; Pfohl, S.; et al. 2023a. Large language models encode clinical knowledge. Nature, 1–9.
- Singhal et al. (2023b) Singhal, K.; Tu, T.; Gottweis, J.; Sayres, R.; Wulczyn, E.; Hou, L.; Clark, K.; Pfohl, S.; Cole-Lewis, H.; Neal, D.; et al. 2023b. Towards expert-level medical question answering with large language models. ArXiv preprint, abs/2305.09617.
- Sun et al. (2023a) Sun, T.; Zhang, X.; He, Z.; Li, P.; Cheng, Q.; Yan, H.; Liu, X.; Shao, Y.; Tang, Q.; Zhao, X.; Chen, K.; Zheng, Y.; Zhou, Z.; Li, R.; Zhan, J.; Zhou, Y.; Li, L.; Yang, X.; Wu, L.; Yin, Z.; Huang, X.; and Qiu, X. 2023a. MOSS: Training Conversational Language Models from Synthetic Data.
- Sun et al. (2023b) Sun, Z.; Shen, Y.; Zhou, Q.; Zhang, H.; Chen, Z.; Cox, D.; Yang, Y.; and Gan, C. 2023b. Principle-driven self-alignment of language models from scratch with minimal human supervision. ArXiv preprint, abs/2305.03047.
- Touvron et al. (2023) Touvron, H.; Lavril, T.; Izacard, G.; Martinet, X.; Lachaux, M.-A.; Lacroix, T.; Rozière, B.; Goyal, N.; Hambro, E.; Azhar, F.; et al. 2023. Llama: Open and efficient foundation language models. ArXiv preprint, abs/2302.13971.
- Wang et al. (2023a) Wang, H.; Liu, C.; Xi, N.; Qiang, Z.; Zhao, S.; Qin, B.; and Liu, T. 2023a. Huatuo: Tuning llama model with chinese medical knowledge. ArXiv preprint, abs/2304.06975.
- Wang et al. (2023b) Wang, P.; Li, L.; Chen, L.; Zhu, D.; Lin, B.; Cao, Y.; Liu, Q.; Liu, T.; and Sui, Z. 2023b. Large language models are not fair evaluators. ArXiv preprint, abs/2305.17926.
- Wang et al. (2023c) Wang, Y.; Kordi, Y.; Mishra, S.; Liu, A.; Smith, N. A.; Khashabi, D.; and Hajishirzi, H. 2023c. Self-Instruct: Aligning Language Models with Self-Generated Instructions. In Proceedings of the 61st Annual Meeting of the Association for Computational Linguistics (Volume 1: Long Papers), 13484–13508. Toronto, Canada: Association for Computational Linguistics.
- Wei et al. (2022) Wei, J.; Bosma, M.; Zhao, V. Y.; Guu, K.; Yu, A. W.; Lester, B.; Du, N.; Dai, A. M.; and Le, Q. V. 2022. Finetuned Language Models are Zero-Shot Learners. In The Tenth International Conference on Learning Representations, ICLR 2022, Virtual Event, April 25-29, 2022. OpenReview.net.
- Xiong et al. (2023) Xiong, H.; Wang, S.; Zhu, Y.; Zhao, Z.; Liu, Y.; Wang, Q.; and Shen, D. 2023. Doctorglm: Fine-tuning your chinese doctor is not a herculean task. ArXiv preprint, abs/2304.01097.
- Yunxiang et al. (2023) Yunxiang, L.; Zihan, L.; Kai, Z.; Ruilong, D.; and You, Z. 2023. Chatdoctor: A medical chat model fine-tuned on llama model using medical domain knowledge. ArXiv preprint, abs/2303.14070.
- Zhang et al. (2023) Zhang, H.; Chen, J.; Jiang, F.; Yu, F.; Chen, Z.; Li, J.; Chen, G.; Wu, X.; Zhang, Z.; Xiao, Q.; et al. 2023. HuatuoGPT, towards Taming Language Model to Be a Doctor. ArXiv preprint, abs/2305.15075.
- Zhang et al. (2022) Zhang, J.; Gan, R.; Wang, J.; Zhang, Y.; Zhang, L.; Yang, P.; Gao, X.; Wu, Z.; Dong, X.; He, J.; Zhuo, J.; Yang, Q.; Huang, Y.; Li, X.; Wu, Y.; Lu, J.; Zhu, X.; Chen, W.; Han, T.; Pan, K.; Wang, R.; Wang, H.; Wu, X.; Zeng, Z.; and Chen, C. 2022. Fengshenbang 1.0: Being the Foundation of Chinese Cognitive Intelligence. CoRR, abs/2209.02970.
- Zhao et al. (2023) Zhao, W. X.; Zhou, K.; Li, J.; Tang, T.; Wang, X.; Hou, Y.; Min, Y.; Zhang, B.; Zhang, J.; Dong, Z.; et al. 2023. A survey of large language models. ArXiv preprint, abs/2303.18223.
- Zheng et al. (2023) Zheng, L.; Chiang, W.-L.; Sheng, Y.; Zhuang, S.; Wu, Z.; Zhuang, Y.; Lin, Z.; Li, Z.; Li, D.; Xing, E.; et al. 2023. Judging LLM-as-a-judge with MT-Bench and Chatbot Arena. ArXiv preprint, abs/2306.05685.
- Zhou et al. (2023) Zhou, C.; Liu, P.; Xu, P.; Iyer, S.; Sun, J.; Mao, Y.; Ma, X.; Efrat, A.; Yu, P.; Yu, L.; et al. 2023. Lima: Less is more for alignment. arXiv preprint arXiv:2305.1120.
- Zhu and Wang (2023) Zhu, W.; and Wang, X. 2023. ChatMed: A Chinese Medical Large Language Model. https://github.com/michael-wzhu/ChatMed.
Appendix A Evaluation Template
When using AI evaluation, we choose the following prompt template in Table 3 to interact with GPT-4. The safety evaluation results output by GPT-4 are only for experts’ reference when making decisions, in order to save manpower, if there are enough medical experts, the part about safety can be deleted.
|
As a referee, please evaluate the following two responses to the same medical question. ””” **Question**: [Question content] **Response1**: [Content of Response1] **Response2**: [Content of Response2] ””” The evaluation criteria, prioritized in order, include Safety, Professionalism, and Fluency, the specific definition is as follows:. **Evaluation Criteria**: 1. **Safety**: - Provide scientific, accurate medical knowledge. - Admit ignorance for unknown knowledge. - Ensure patient safety; refuse information or suggestions that might cause harm. - Adhere to medical ethics and respect patient choices. 2. **Professionalism**: - Accurately understand patient questions and provide relevant answers. - Clearly and concisely explain complex medical knowledge. - Proactively inquire about the patient’s condition when necessary. 3. **fluency**: - Ensure semantic coherence with no logical errors or irrelevant information. - Maintain consistency in style and content. - Maintain a friendly, enthusiastic answering attitude. **Note**: Evaluate based on the importance of **Safety Professionalism fluency**. If there is a conflict, prioritize the former. **Output Format**: Based on the above criteria, judge the result of “Answer1” relative to “Answer2”. Output as: Win, Lose, or Tie. |
Appendix B Training Settings in every stage
| Pretrain | SFT | RM | PPO | |
|---|---|---|---|---|
| Learning Rate |
5e-5 |
7e-5 |
1e-4 |
5e-5 |
| Lora Rank |
- |
16 |
16 |
16 |
| Epochs |
4 |
3 |
10 |
2 |
| Batch Size |
16 |
16 |
32 |
8 |
| Accumulation |
4 |
4 |
4 |
4 |
| Time |
103 hours |
67 hous |
5 hours |
46 hours |
Appendix C Dialogue Cases
|
User:
|
|---|
|
BenTsao
|
|
DoctorGLM
|
|
HuatuoGPT
|
|
ChatGPT
|
|
User-1:
|
|---|
|
Zhongjing-LLaMA-1
|
|
User-2
|
|
Zhongjing-LLaMA-2
|
|
User-3
|
|
Zhongjing-LLaMA-3
|